



Commentary by Macaulay Ojeaga, MD on the article: Liang J, Lin SY. Tapering Biologic Therapy in Chronic Rhinosinusitis With Nasal Polyps. JAMA Otolaryngol Head Neck Surg. 2026 Feb 1;152(2):115-116. doi: 10.1001/jamaoto.2025.4675. PMID: 41452610. Biologic therapy has transformed the management of…
Top 3 Things to Know About Allergy and Migraines
9.
Top 3 Things to Know About Allergy and Migraines
As Migraine and Headache Awareness Month is winding down, we are sharing the top insights into the relationship between migraine and allergy for your practice extracted from “Sinus Headache, Migraine, and Allergy” presented at the 2024 AAOA Annual Meeting by Mark E. Mehle, MD, FACS, Assistant Clinical Professor, Northeast Ohio Medical University.
Q: How do you differentiate if a patient has migraine or rhinogenic headache?
A: To differentiate a sinus headache complaint from rhinogenic headache, your standard questionnaire for your rhinology patients can screen for migraine.
According to the International Headache Society Criteria for Migraine, Migraine is an episodic recurrent headache lasting 4-72 hours with:
Any two (2) of these pain qualities:
- Unilateral pain
- Throbbing pain
- Pain worsened by movement
- Moderate or severe pain
AND
Any one (1) of these associated symptoms:
- Nausea
- Vomiting
- Photophobia and phonophobia
Q: Why do patients with migraines think they have sinus headaches?
A: A sinus headache is a complaint, not a diagnosis. In the sinus-like presentation of migraine, pain and pressure can be felt in or near eyes and sinuses, and the five seven reflex arc trigeminal nerve to facial nerve, the superior salvatory nucleus of seven triggers the stuffy, snotty nose. The timing is also important: Migraines last 4-72 hours. Sinus patients with acute sinusitis or chronic rhinosinusitis don’t have a lot of pain, and they have 10-14 days or 12 weeks of symptoms, respectively.
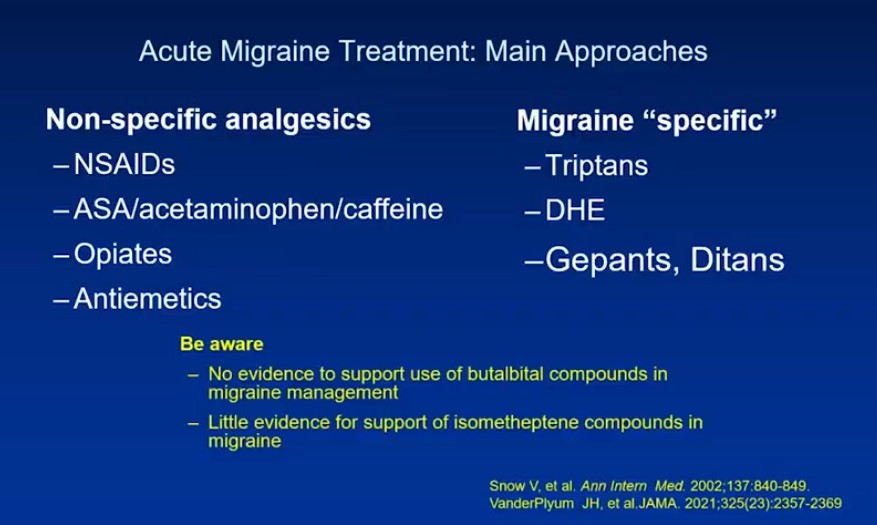
Q: How do you treat migraine? How do we sort out the allergy component? Is allergy treatment beneficial for these patients with migraine and allergy in a global sense or just for the allergy symptoms?
A: First, screen the patient for migraine as the symptoms are significantly different from rhinogenic pain. Radiographic studies (CT) may be helpful, but not reliable, in the case of migraine.
Making sure not to over-operate for pain. Recognize there may be a link between allergy and migraine, if they have sinonasal disease. According to Eross (2007), sinus headache migraines can be triggered by weather changes, seasonal variations, and exposure to allergens, even if the patient had a negative skin test.
For the latest on migraine management, join us in Oceanside for the 2025 AAOA Annual Meeting November 14-16.
Register here: https://www.aaoallergy.org/education/aaoa-annual-meeting-2025/
Sources:
Altonji S, Del Risco A, Kilpatrick KW, Kuchibhatla M, Hachem RA, Jang DW. Predictors of non-rhinogenic facial pain or pressure in otolaryngology clinic. Otolaryngol Head Neck Surg. 2024; 170(5):1314-1318. doi: 10.1002/ohn.644
Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition (beta version). Cephtalalgia. 2013; 33:629-808. doi: 10.1177/0333102413485658.
Headache Classification Committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephtalalgia. 2018; 38:1-211. doi:10.1177/0333102417738202
Eross E, Dodick D, Eross M. The sinus, allergy and migraine study (SAMS). Headache. 2007; 47(2):213-224. doi: 10.1111/j.1526-4610.2006.00688.x
International Headache Society. Guidelines/ICHD. 2020. URL: https://ihs-headache.org/en/resources/guidelines/
Mehle M, Kremer P. Sinus CT scan findings in “sinus headache” migraineurs. Headache. 2008; 48(1):68-71. doi: 10.1111/j.1526-4610.2007.00811.x.
Schreiber CP, Hutchinson S, Webster CJ, Ames M, Richardson MS, Powers C. Prevalence of migraine in patients with a history of self-reported or physician-diagnosed “sinus” headache. Arch Intern Med. 2004;164(16):1769-1772. doi:10.1001/archinte.164.16.1769
From “Sinus Headache, Migraine, and Allergy” at 2024 AAOA Annual Meeting by Dr. Mark E. Mehle, MD, FACS, Assistant clinical Professor, Northeast Ohio Medical University.
The American Academy of Otolaryngic Allergy (AAOA) Practice Resources are intended as a guide to help AAOA members integrate allergy into their otolaryngology practice and to continually improve on this integration as new information, regulations, and resources become available.
While these tools are meant as resources, we highly recommend seeking input from your practice counsel and local/state medical associations and regulatory authorities, as rules vary between states. Each practice is responsible for confirming coverage, coding, and payment parameters for those payers and regulators affecting their practice. Our intention is to offer insights by sharing what others within AAOA do. These are not meant as recommendations.